In 1981, David A. Jenkins, M.D., Ph.D., DSc., Department of Nutrition Sciences at Canada's University of Toronto, first published an article describing the Glycemic Index in The American Journal of Clinical Nutrition. He then formulated the Glycemic Index (GI) food by food, with numerical values assigned (Jenkins et al, 1981) as they pertained to the consumption of sugar and more recently, a piece of white bread.

The main theory is that the Glycemic Index is simply an extension of the 1977 Fiber Hypothesis of Burkitt and Trowell, which holds that dietary fiber is absorbed slowly and may have metabolic effects that are beneficial, particularly for prevention of diabetes and cardiac disease.
In the 1990's, the concepts of central abdominal adiposity and metabolic syndrome (Bjorntorp, 1992), intraabdominal fat, high waist:hip ratio (Landin et al, 1990), and insulin resistance (Vague and Raccah, 1992) were also being formed. Foods that lead to a higher blood glucose and insulin level have a higher numerical GI value. This numerical system is essential to decreasing the physiologic response, and to the prevention and treatment of diabetes and other chronic diseases. Charting can be done by GI itself as a numerical value, or by grouping the Category of GI (See Chart).
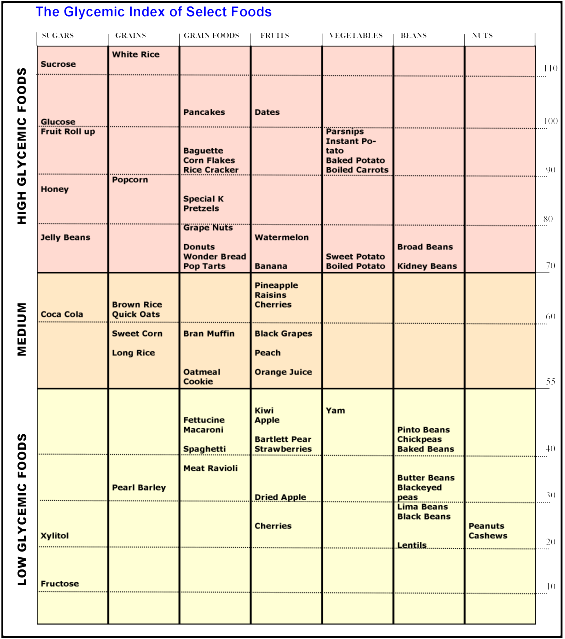
Chart. High, Medium, and Low-Glycemic Foods.
The typical Western diet hits the body with starchy carbohydrates in the morning, in the afternoon, and again in the evening. After eating, the blood glucose increases and to compensate, the blood insulin levels also increase. The problem is not just the resulting hyperglycemia; it is the hyperinsulinemia also. When insulin is chronically elevated due to a high-glycemic index diet, fat can not be utilized, the body becomes insulin-resistant, and elevated insulin levels no longer drive glucose into the cells. Diabetes and central adiposity ensue, with the attendant increase in cardiac risk.
The low-glycemic index diet has been attributed with the following:
2. In subjects with diabetes, decreased blood glucose levels;
3. In subjects with hyperlipidemia, decreased lipid levels;
4. Increased HDL levels (beneficial lipids);
5. Decreased risk of diabetes;
6. Decreased risk of cardiovascular events;
7. Decreased risk of colon cancer;
8. Decreased risk of breast cancer;
9. Decreased central obesity.
Most recently,
1. In overweight and obese women with polycystic ovary syndrome, the low-glycemic index diet increased insulin sensitivity (less diabetes tendency) and decreased high-sensitivity C-reactive Protein (decreased inflammatory marker) (Mehrabani HH, et al, 2012);
2. In Canadians with cancer, a higher GI and GL diet increased the risk of the following cancers: prostate, colorectal, rectal, and pancreatic ( Hu J, et al, 2012);
While the low-glycemic index diet and was first described in 1981, its popularity began to abound in the 1990's. Here it is now 2012, and we estimate that millions of women have not heard of it. We hope to initiate change in this matter, as it is time to decrease abdominal obesity, diabetes, and the attendant morbidity and mortality associated with diet as a causative factor.
We say, "It's about time."
Stay tuned for more.
by Margaret Aranda Ferrante, M.D.
References
Bjorntorp P. Abdominal obesity and the metabolic syndrome. Ann Med 1992 Dec; 24(6):465-8. Abstract
Burkitt DP and Trowell HC. Dietary fibre and western diseases. Ir Med J, 1977 June 18; 70(9):272-7. Medline
Hu J, et al, the Canadian Cancer Registries Epidemiology Research Group. Glycemic index, glycemic load and cancer risk. Ann Oncol. July 25. (Epub ahead of print). Medline
Jenkins DJ, et al. Glycemic index of foods: a physiological basis for carbohydrate exchange. Am J Clin Nutr. 34; 362-366.
Jenkins DA, et al. Glycemic index: overview of implications in health and disease. Am J Clin Nutr 2002 July; 76(1):266S-73S. View Full Article Here
Landin K, et al. Increased insulin resistance and fat cell lipolysis in obese but not lean women with a high waist/hip ratio. Eur J Clin Invest. 1990 Oct;20(5):530-5. Medline
Mehrabani HH et al. Beneficial effects of a high-protein, low-glycemic-load hypocaloric diet in overweight and obese women with polycystic ovary syndrome: a randomized controlled intervention study. J Am Coll Nutr. 2012 Apr;31(2):117-25. Medline
Vague P and Raccah D. The syndrome of insulin resistance. Horm Res 1992;38:28-32.
Am J Clin Nutr. 2002 Jul;76(1):266S-73S.
No comments:
Post a Comment
We Love Comments! They help us to Dominate the Internet for Age Management Medicine! Yay!